
FROM: Iowa Fatality Assessment and Control Evaluation (FACE) Program
SUBJECT: Sawmill worker killed while unplugging wood chips from a chipper duct.
SUMMARY:
A 22-year-old male employee died after being caught by a cable while cleaning a wood-chipping machine at a sawmill. The family-owned business had been in operation for several years with about 10 employees, although the number varied throughout the year. The process included discarded wood pieces from the sawmill, which were carried on a conveyor belt and fed into a wood chipper. The discharge chute was attached to a section of round duct, which was used to transport the chipped material into a hopper. The material was collected in a container below the hopper, and removed from the area. On the day of the incident, the round duct became plugged. The victim stood on a platform, and with the assistance of another employee, he removed the access cover on the hopper, and pushed a straight cable into the duct to clean out the duct while the chipper was running. According to the supervisor, the cable was marked with paint, to designate how far the cable could be inserted into the duct. The cable got caught in the chipper and wrapped around the employee’s neck causing him to be thrown off the platform instantaneously. An employee called the local sheriff for assistance using a cellular phone, since there was no phone at the sawmill. The County sheriff, county EMS (Emergency Medical Service), and local fire department Jaws of Life responded to the call. The victim received multiple cervical fractures and died within minutes.
RECOMMENDATIONS based on our evaluation are as follows:
1. Employers should establish an energy control program in accordance with the requirements of 29 CFR 1910.147. The program should include procedures and employee training to ensure that equipment is locked out and rendered inoperative, before any employee performs servicing or maintenance on a piece of equipment.
2. All maintenance tasks should be carried out only when the machine is locked out. Employers should ensure that machinery operates properly and does not require excessive maintenance.
3. Employers should ensure that a job safety analysis has been performed on all work-related tasks.
4. Employers should develop, implement, and enforce a written safety program.
Introduction
At 4:15 PM on July 6, 1998, a 22-year-old male employee died after being caught by a cable while operating a chipper. The Iowa FACE program was notified of the incident by the Iowa Department of Public Health on October 20, 1998. On December 30, 1998, an on-site evaluation was conducted, and a FACE investigator also met with the deputy and county sheriff. Photographs, which were taken by the county sheriff following the incident, were reviewed. At the time of the FACE evaluation, it was noted that several modifications, which were required by the Department of Labor, had been completed at the facility.
The incident occurred at a small rural family-owned sawmill that had been in operation for several years. The facility employed 10 employees throughout the year, although the number varied depending on the workload. The facility did not have an established safety program, safety training, or a lockout / tagout program. The sawmill was in operation throughout the year.
Investigation
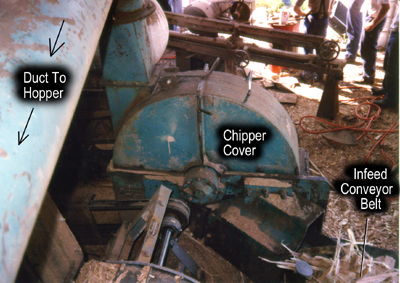
When the mill is operating, logs are sawn into boards outside the mill building. Slabs of wood and bark are discarded into a vibrating conveyor, which feeds into a diesel-powered wood chipper. Chipped material is discharged from the chipper through a duct and into a hopper located inside the mill building. The material is then loaded into containers and removed from the area. During normal operation hours of operation the conveyor and chipper operated continuously.
The chipper, purchased used and installed about a year before
the incident, consists of an infeed chute, a shrouded chipper
wheel, and a discharge chute. During operation, the wheel rotates
at 900 revolutions per minute (rpm). Material is chipped by 3
knives mounted on the wheel and discharged through into a 12-inch
round duct by 3 steel paddles mounted on the outer surface of
the wheel. The chipped material travels through the duct for 11
feet and into the hopper. During normal hours of operation the
conveyor and chipper operated continuously. About once a month
the discharge duct would plug with chips. Because the chipper
was not equipped with an emergency shutoff, the entire operation
would have to be shut down so that the duct could be cleared.
When the duct became plugged with wood chips, the employees were
instructed to use a straight cable 28 feet in length and 5/8 inch
in diameter to clear the plug. The victim was familiar with operating
the chipper, and had cleaned or unplugged the chipper several
times. According to the supervisor, the cable had been marked
with paint, to designate how far the cable should be inserted
into the duct. During the evaluation, it was noted that the painted
mark was worn off the cable and no longer visible.
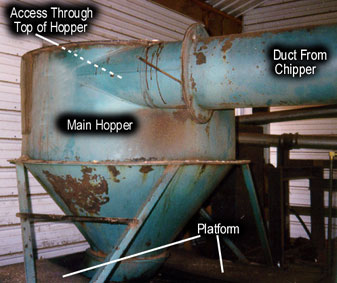 On the day of the incident, the duct had plugged,
and the entire operation had been shut down. The victim climbed
onto a platform (about 4 feet high) and took the straight cable
to unplug the duct. He had the cable laying over his shoulder
and was feeding it into the duct. Another employee assisted him
by climbing inside the main hopper to help push the cable through
the duct. The employees were able to make a hole in the wood chips
and pulled the cable back out. The supervisor saw the employee
on the platform and walked by the area, tugged the victim on the
pant leg and shouted to remind him to watch for the paint marking
on the straight cable. The victim acknowledged this and then turned
the chipper back on to help unplug the pipe and shoved the cable
into the pipe again. The cable caught in the chipper, and wrapped
around the victim’s neck throwing him off the platform. The
victim received multiple cervical fractures, and died instantly.
The other employee that was assisting him received minor lacerations.
An employee called the local sheriff for assistance using a cellular
phone, since there was no phone at the sawmill. The local sheriff,
county EMS, and local fire department responded to the call.
On the day of the incident, the duct had plugged,
and the entire operation had been shut down. The victim climbed
onto a platform (about 4 feet high) and took the straight cable
to unplug the duct. He had the cable laying over his shoulder
and was feeding it into the duct. Another employee assisted him
by climbing inside the main hopper to help push the cable through
the duct. The employees were able to make a hole in the wood chips
and pulled the cable back out. The supervisor saw the employee
on the platform and walked by the area, tugged the victim on the
pant leg and shouted to remind him to watch for the paint marking
on the straight cable. The victim acknowledged this and then turned
the chipper back on to help unplug the pipe and shoved the cable
into the pipe again. The cable caught in the chipper, and wrapped
around the victim’s neck throwing him off the platform. The
victim received multiple cervical fractures, and died instantly.
The other employee that was assisting him received minor lacerations.
An employee called the local sheriff for assistance using a cellular
phone, since there was no phone at the sawmill. The local sheriff,
county EMS, and local fire department responded to the call.
Following the incident and subsequent OSHA investigation, several changes were instituted at the sawmill. A safety program was initiated with general safety training and training specific to lockout / tagout procedures. A lockout / tagout program was implemented which included instruction for the employees on how to safely turn off the chipper whenever the duct became plugged. Tags were attached to the equipment to identify the machine specific lockout procedures. An access panel or clean-out port, was installed in the duct to facilitate easier cleaning. A grate was welded to the top of the main hopper to prevent access.
Although the weather was hot and humid in July, environmental conditions were not a contributing factor in the incident.
Cause of Death
The immediate cause of death was a spinal cord transection due to multiple cervical fractures.
Discussion: The standard requires employers to isolate the machine from its energy source before maintenance, and when an employee works at the in-feed / discharge area to unclog the chipper. The energy control program should include step-by-step procedure and documentation. In this case, machine access covers and doors should not be opened, or the machine should not be maintained while it is running. When pushing clogged wood chips, there was a danger that the cable would reach the chipper and may cause serious injury to the worker.
Discussion: The wood chipper in this case had become clogged frequently. A clean out system had been devised, which included using a long steel cable to push the clogged wood chips while the machine was running. This procedure was dangerous because the steel cable could easily be pushed too far into the chipper blades, as happened in this case. It appeared that the clogging was a frequent event, and therefore the chipper discharge did not function properly. This could be due to poor machine design such as, bends in the discharge pipe, restricted airflow, or other problems. To ensure safety, it is important to ensure that machinery is in good working order, and does not require excessive maintenance.
Discussion: Job safety analysis (JSA) is a procedure used to review methods or steps for a particular task in order to identify potential hazards. Employees are encouraged to participate in job safety analysis. The task can be broken down to a sequence of steps or actions, which are used to identify hazards connected to the task or produced by the environment. Once the hazards are known, the proper solutions can be developed to eliminate or control hazards. In this case, a job safety analysis may have identified the hazard of removing the access door and inserting the cable. Modifications could have been made to eliminate the hazard.
Discussion: The employer had no written safety program, or safe work procedures. The implementation and enforcement of a comprehensive safety program should include task-specific safety procedures and employee training. Training is a critical element in an integrated safety program and should include the communication of task-specific safety procedures and training in the avoidance and abatement of these hazards. Employees should have the knowledge, training and experience to perform the job that he/she is designated. Knowledge and competency are normally achieved through training or experience or a combination of both. Every new employee should work under the close supervision of a designated person until the employee is able to demonstrate the ability to safely perform the new job independently. In this case, there was no written safety program or safe work procedures. A safety program should provide the employee with training on task-specific safety procedures.
____________________________________________________________________________
| Lois Etre PhD. | Wayne Johnson MD. |
| Industrial Hygienist/Investigator | Chief Trauma Investigator |
| Institute for Rural & Environmental Health | Institute for Rural & Environmental Health |
| The University of Iowa -- Iowa City, Iowa | The University of Iowa -- Iowa City, Iowa |
References
29 CRF 1910.147 The Control of Hazardous Energy (Lockout/Tagout).
OSHA Logging Advisor, Processing at the Yard.
OSHA Compliance Directive, CPL 2-1.19.